Brighton & Hove Palliative and End of Life Care (PEoLC) ICT Profile
February 2026
Introduction
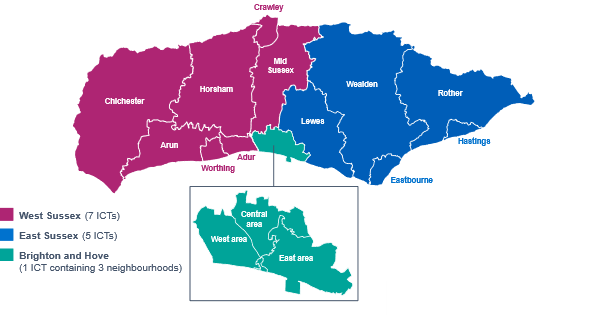
There are 13 Integrated Community Teams (ICTs) across Brighton & Hove, East and West Sussex, with Brighton & Hove containing 3 neighbourhoods.
The ICT Programme have implemented an ICT Data Group, enabling ICB, Public Health, Local Authority, VCSE and wider stakeholders to meet and collaborate regularly in the development and design of Sussex ICT data core profiles.
The Sussex ICT model will be driven by data and reflective of population needs. To do this effectively, ICTs need to access a variety of data sets that enable them to understand their local demographics, health needs, social determinants and wider determinants of health.
This Palliative and End of Life Care data and needs data pack is designed to complement and be used alongside other system data and information.
The ICT profiles were intended to set the scene for the ICTs. Whilst they alone will not provide the final answer, they are designed to help stimulate the questions which will. After initial release in December 2023, the packs will develop further in response to feedback to help support the ICTs in their development.
The ICT profile for Brighton & Hove is available from ICT Profiles, and the Sussex Palliative and End of Life Care Needs Assessment will be published in the summer of 2026.
Sussex ICTs and neighbourhoods
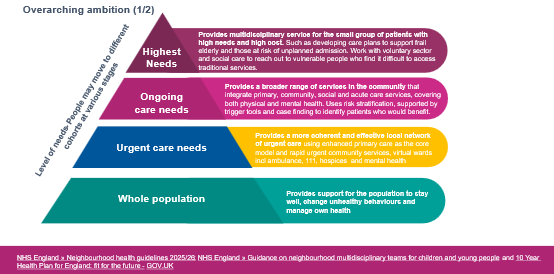
Our model for health, care and wellbeing
Sussex data and national evidence
Sussex data and national evidence
The recorded prevalence of registered patients on the palliative and supportive care register is 0.54% (2024/25). There is variation between ICTs, ranging from 0.19% to 0.91%. (QoF)
53% of people on the palliative care register have a ReSPECT Plan recorded. It ranges from 35% to 66% for ICTs and is lower in non-white groups (39%) compared to White groups (53%) (SID)
13% of people on the palliative care register have an Advance Care Plan recorded. There is a variation between ICTs from 3% to 26%. (SID)
31% of people on the palliative care register have a preferred place of death recorded. There is a variation between ICT from 13% - 44%. (SID)
37% of adults (18+ years) died in hospital, 29% in a care home, 36% at home, 6% in a hospice and 2% in other places. (2022-2024, ONS). National evidence suggests most people want to die at home, in comfort, if possible (Marie Curie)
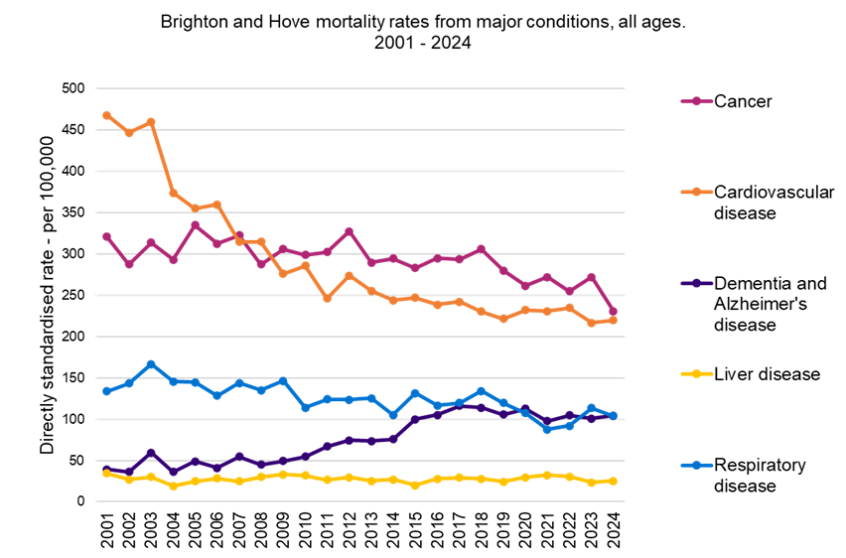
Cancer is a leading cause of death (14,963 / 26%), followed by CVD (13,999 / 25%), dementia and Alzheimer's disease (7,250/ 13%) and respiratory 6,259 (11%) (2022-2024, 18+ years, ONS)
Carers may be involved in providing PEoLC. Unpaid carers range from 7.5% - 10.0% of the population at ICT level (Census 2021)
National evidence shows people with conditions other than cancer and people from economically and socially deprived areas, ethnic minority communities and LGBT people can experience barriers to accessing end-of-life care services (NICE, 2019). Other evidence highlights that those with Learning Difficulties can also experience inequalities at the end of their life (NHS E 2022)
Non-white ethnic groups are more likely to attend hospital accident and emergency departments in the last 90 days of life compared to their White peers (2024/25, NHS ICB Palliative End of Life Care Dashboard)
Dementia is often not recognised as a terminal diagnosis, which can lead to poor access to care. (Marie Curie)
Brighton & Hove's ICTs - Key data on Palliative and End of Life Care
SID-QOF register, 2024/25
Brighton & Hove:
0.28% of registered patients are on the palliative care register (0.54% for Sussex)
51% of people on the palliative care register have a ReSPECT Plan recorded (53% for Sussex)
14% percentage of people on the palliative care register have an Advance Care Plan recorded (13% for Sussex)
70% percentage of people on the palliative care register are residing at home (67% for Sussex)
34% of people on a palliative care register have a record of their preferred place of death (31% for Sussex)
7.5% of people are unpaid carers
SID – QOF: The SNOMED codes & QoF business rules have been used to analyse the SID data relating to Palliative Care Registers. There are limitations to the SID data we’ve published, and this is not identical to the QoF data. At the time of analysis, a small number of practices weren’t participating in the SID in 2025.
Understanding what people die from is vital for shaping effective end-of-life care. It helps identify common conditions, anticipate patient needs, and allocate resources appropriately. This knowledge ensures care is person-centred, reduces unnecessary interventions, supports families, and guides planning to improve dignity, comfort, and quality in the final stages of life.
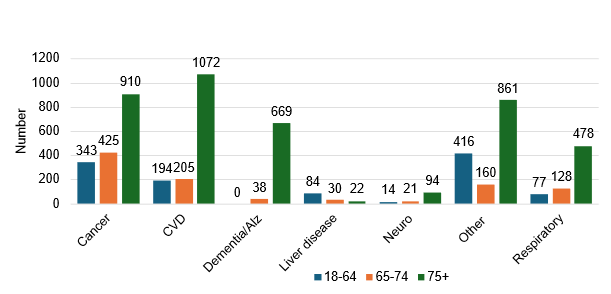
Cancer (27%) and CVD (24%) are the leading causes of death (2022-24, ONS)
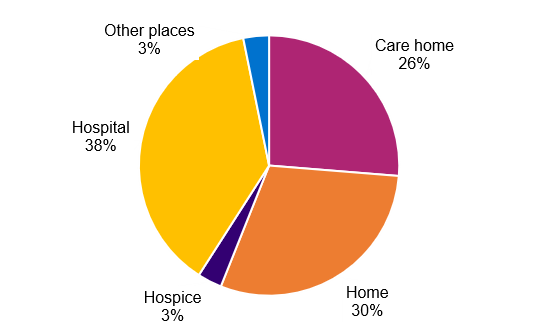
38% of people died in a hospital (2022-24, ONS)
30% of people died at home (2022-24, ONS)
26% died in a care home (2022-24, ONS)
Dementia, as a leading cause of death, has been increasing since 2010 (DHSC)
The number of deaths that may require PEoLC will rise from 1,980 in 2024 to 2,250 in 2044 (ESCC)
90% of deaths in Sussex are likely to require PEoLC (Marie Curie)
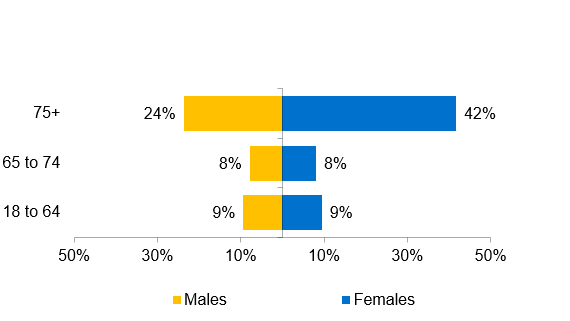
Brighton & Hove Age and Sex distribution of people on the Palliative Care SID-QOF register, 2024 to 2025
Brighton & Hove place of death (2022 to 2024, ONS)
Brighton & Hove underlying cause of death and age group
‘Other’ includes deaths by accidents, poisonings, suicides and other causes that aren’t included and grouped into the major conditions such as Cancer, CVD, Dementia, Respiratory, etc.
Opportunity areas
1. Increase Advance Care Planning (ACP) discussions, ReSPECT processes and the recording of these in Brighton & Hove
Why: Only 51% of people on the Palliative Care Register have a ReSPECT Plan recorded, whilst 34% of the same people have stated their preferred place of death, and just 14% have an Advance Care Plan recorded.
Improving ACP ensures care aligns with patient wishes, reduces unwanted hospital admissions, and supports a “good death” at home or in the preferred setting where possible.
2. Strengthen data integration and use
Why: The ICT model is designed to be data-driven and reflective of local population needs. Enhanced data sharing and integration across NHS, Public Health, Local Authority, and VCSE partners will enable more accurate identification of needs, better service planning, and targeted interventions for Brighton & Hove and other Sussex ICTs in the future.
3. Expand community-based and home care services
Why: National evidence and local data show most people want to die at home, yet 38% die in hospital in Brighton & Hove. Expanding community and home-based palliative and end-of-life care will help more people achieve their preferred place of death and may reduce pressure on hospitals.
4. Identify, involve and support families and carers
Why: Families and carers play a vital role but often experience negative health, financial and social outcomes. Identifying, involving and providing practical, emotional and bereavement support helps carers cope, reduces stress, and improves the overall quality of end-of-life care.
5. Use the end-of-life care for adults guidance and tailor services to local demographics and PEoLC needs
Why: Services must be tailored to reflect these demographics, morbidities and conditions that lead and contribute to death, address inequalities for ethnic minorities, LGBTQ+ people and people with limited health literacy to ensure equitable access to high-quality palliative and end-of-life care for all groups.
Improving Palliative and End of Life Care in Brighton & Hove
Improving Palliative and End of Life Care in Brighton & Hove will enable the following:
A good death
A good death (or good end-of-life experience) is defined as having the right care, support, and systems in place, so that people feel protected and safe, and their carers and loved ones understand what support is available.
National evidence suggests most people want to die at home.
Role of professionals
The ability of all health and care professionals to recognise when someone is entering the last year of life and to discuss end of life openly, honestly and sensitively is essential to appropriate end of life care.
Improved symptom management
End-of-life and palliative care ensure effective management of pain and other distressing symptoms, helping people live as well as possible in line with their wishes.
Emotional and spiritual support is important
Care extends beyond physical needs, providing emotional and spiritual support to patients and those close to them, which is crucial for feeling safe and supported during a difficult time.
Personalised, holistic care
Services are tailored to what matters most to each individual, enabling people to spend quality time with loved ones and, where possible, die in their preferred place and manner.
Coordinated and accessible services, and Advanced Care Planning
Joined-up health and social care systems reduce stress for patients and families, making it easier to access the right support and focus on important things at the end of life. Understanding when people and their families no longer wish for healthcare interventions is also an improvement. Advance Care Planning and ReSPECT Plan enable this.
Support for families and carers
Palliative care provides practical, emotional, and bereavement support for families and carers, helping them cope with the challenges and grief associated with end-of-life care.