Introduction
Definitions
Brighton & Hove’s Joint Strategic Needs Assessment programme is committed to the Social Model of Disability, developed over the last 40 years by disabled people and differentiates between 'impairment' (functional limitations of the mind, body, or senses) and 'disability' (disadvantages or restrictions imposed by society).
Some people find the term "impairment" deeply offensive, as it suggests being "less than" or different from a perceived norm. When applying the Social Model, it is advisable to avoid this term and instead focus on identifying barriers to access.
A central idea of the Social Model is that societal arrangements disable people; if these arrangements were different, individuals would be enabled with their functional differences. The Social Model defines disability as "the loss or limitation of opportunities to participate in the normal life of the community on an equal level with others due to physical or social barriers." This definition emphasises the importance of removing barriers that hinder disabled people's full participation as citizens.
It is important to acknowledge that for some individuals who identify as disabled, the medical model is significant, as they seek better support for their long-term, potentially fluctuating health conditions.
The Equality Act 2010 defines disability as a physical or mental impairment that has a substantial and long-term (lasting 12 months or more) negative effect on a person's ability to perform normal daily activities.
Sensory disabilities include D/deaf and hearing loss, blindness, vision loss or a combination of these. This summary JSNA aims to use the term sensory loss, needs or requirements to reflect the Social Model of Disability. However certain data sets use different terms that may be used in the data figures and tables. There are several terms used to describe deaf individuals, and it is best to use the terminology preferred by the people we are working with.
Hearing loss
In the UK, the term ‘deaf’ (lower case) generally refers to the audiological condition of hearing loss at all levels. People who describe themselves as deaf are likely to be profoundly deaf. People who have retained a considerable degree of hearing might refer to themselves as partially deaf or to their level of hearing as mild to moderate.
"Deaf" (with a capital D) typically refers to people who view themselves as culturally deaf, identify with Deaf culture and as part of Deaf community, and use sign language as their primary means of communication.
"Hard of hearing" or ‘deafened’ (the term more common amongst older people) is widely accepted and used by many people with partial hearing loss.
Terms that should generally be avoided include 'the deaf', which defines people through their disability and also 'hearing impaired' which is often used by medical professionals but can be disliked by many D/deaf people who do not view themselves as having an impairment.
The Deaf Cultural Model is similar to the Social Model of Disability in that it rejects the medical definition of deafness as a loss or impairment. However, the Deaf community sometimes diverges from the Social Model regarding the term "impairment." For most culturally Deaf individuals, there is no "impairment" or "hearing loss." What makes the British Sign Language (BSL) Deaf community unique is its campaign to be recognised as a linguistic minority and the capital "D" is used to signify their campaign for cultural and linguistic recognition.
Strategic context
National
The Department of Health and Social Care’s Fit for the Future: 10 Year Health Plan for England sets out 3 big shifts; from hospital to community, analogue to digital, sickness to prevention. It includes recognition of the needs for people with sensory loss so that deaf people will be supported through British Sign Language accessibility, and blind and visually impaired people supported through screen readers to facilitate people to access and use healthcare on their own terms and:
- ‘My Specialist’ tool where patients can self-refer to specialist care online where clinically appropriate. The RNID proposes this may provide opportunities to include support and follow-up in adjusting to hearing aids, potential use of otoscope images analysed by AI, embed hearing checks and integrate video relay services, enabling people who are deaf to video call an interpreter.
- In the shift from hospitals to neighbourhood settings, hospital eye care records and images will be shared with primary care high street optometrists to tackle ophthalmology waiting lists, a proposal welcomed by the RNIB.
No NHS national plans specifically address the key issues effecting people with hearing loss or who are deaf or for eye health. NICE have a detailed best practice quality statement for hearing loss and serious eye conditions and a range of technology appraisals and clinical guidance:
The British Deaf Association has a 10-Year Strategic Vision 2022 to 2032 focused on transforming the way British Sign Language (BSL) is accessed by deaf children, their families and deaf adults. The RNID sets out annual priorities.
A multi-sector partnership ‘The Eyes Have It (2023)’ report makes recommendations including ensuring people living with sight-threatening conditions are supported by trained Eye Care Liaison Officers, greater utilisation and upskilling of the primary eye care workforce to deliver more care outside hospital:
The NHS Core20PLUS5 is a national approach to reduce healthcare inequalities identifies 5 clinical areas requiring accelerated improvement. For adults the identification of undiagnosed hypertension and support to stop smoking may help reduce later life vision problems. The Core20PLUS5 for children and young people includes a focus on improving care for those with diabetes especially those from disadvantaged communities. Diabetes related retinopathy is one of the leading causes of blindness in later life.
Local
Brighton & Hove City Council’s Plan ‘A Better Brighton & Hove’ sets out its commitment to be inclusive, accessible and fair – a place where everyone can thrive and has an Accessible City Strategy setting out actions to make the city suitable for people with additional sensory needs.
The Joint Health and Wellbeing Strategy 2019 to 2023 covers the life course. Starting Well includes whole family support to prevent problems escalating. Living Well includes disabled people and long-term conditions being supported into work. Ageing Well includes supporting people to live independently in the community by connecting them with their communities to maintain health and prevent isolation, this is especially important for people living with hearing and sight loss.
Sussex Health and Care Partnership Improving Lives Together Strategy sets out an ambition to reduce health inequalities across the city and support people to maintain their independence as they age. The strategy’s Shared Delivery Plan identifies joined up working across mental health, learning disabilities, autism and physical health for children and young people and a focus on long term conditions including diabetes and obesity services, particularly relevant for this JSNA.
As at summer 2025, the local NHS Sussex changes being planned in response to the 10-year plan reflect the focus on neighbourhood delivery of primary and community care, addressing health inequalities and more collaboration across providers to improve service delivery. This in time will include changes for the additional delivery of certain audiology and optometry services in the community.
Key outcomes measures
The Public Health, Adult Social Care and NHS Outcomes Frameworks set out key indicators that help assess how well services are performing across England. These indicators reflect impacts on people's health, independence, and quality of life, contributing to an understanding of the lived experience of people with sensory loss. These are covered throughout this needs assessment and are listed in Appendix 2.
Prevalence of hearing and sight loss
Hearing loss
National
The Royal National Institute for Deaf People (RNID) and Inclusion London estimates:
- one in three adults in the UK are deaf, have hearing loss or tinnitus
- over 18 million adults in the UK are deaf, have hearing loss or tinnitus
- over half the population aged 55 or more have hearing loss and 80% of people, 70 years and over will have hearing loss
- an estimated 1.2 million adults in the UK have hearing loss severe enough that they would not be able to hear most conversational speech
- the number of people with hearing loss in the UK is estimated to rise to 14.2 million by 2035
- there are between 100,000 to 150,000 BSL users in the UK, of whom 87,000 are deaf, and 27,000 use BSL as their main language
- 1 in 10 Deaf people are born into a Deaf family (where one or more members are BSL users)
- 1 in 10 of those born into a Deaf family might have Deaf children
- the UK Deaf community is international with Deaf sign language users coming from all over the world - recently we have seen a small development of new Deaf migrants setting up support groups
Brighton & Hove
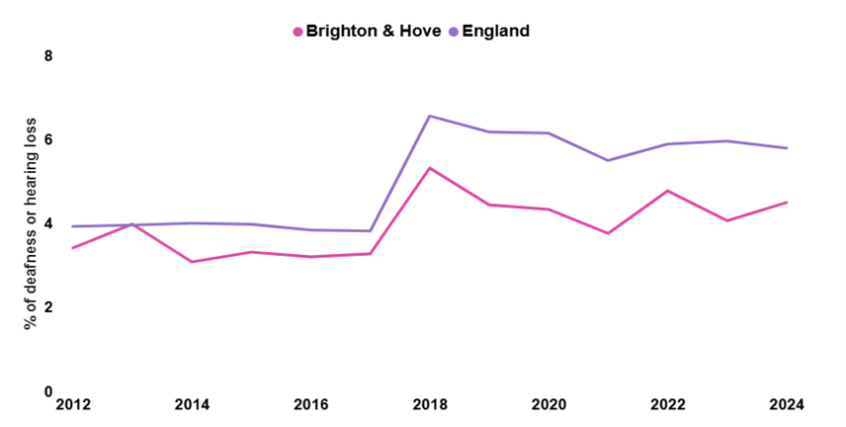
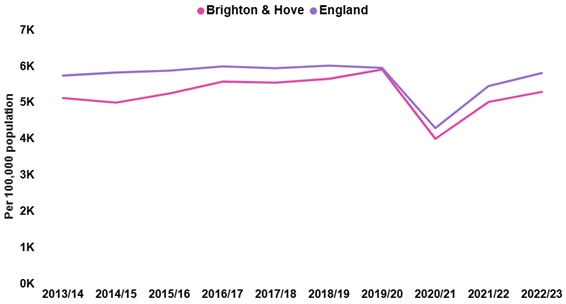
In 2024, 4.5% of people self-reported with deafness or hearing loss in Brighton & Hove, lower than England (5.8%). The rate for both areas has increased since 2012, with England increasing from 3.9% and Brighton & Hove from 3.4% (Figure 1).
Figure 1: Deafness or hearing loss: Percentage of people aged 16 and over self-reporting deafness or hearing loss in Brighton & Hove and England between 2012 and 2024
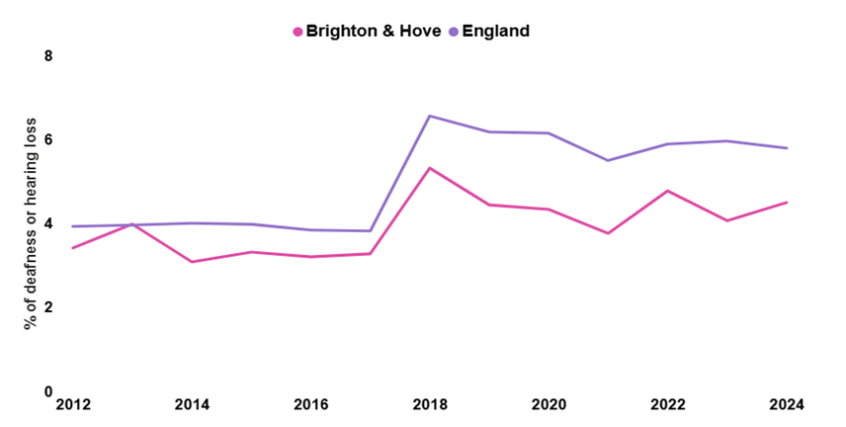
Source: OHID, based on GP-Patient Survey data
In 2023, with the exception of North and Central PCN have between 4 to 5% of people aged 16 years or over reported deafness or hearing loss (Figure 2). In 1.8% in North and Central Brighton PCN it is 2%, with a large number of young people registered at the university practice in this PCN.
All PCNs within Brighton & Hove have a lower rate than England (6.0%), likely due to the younger population in the city compared to England.
Figure 2: Percentage of adults aged 16 year or over with self-reported deafness or hearing loss in Brighton & Hove by Primary Care Network (PCN) and England, 2023
Source: OHID, based on GP-Patient Survey Data, 2023
Data from the 2021 Census shows:
- For 145 Brighton & Hove residents their main or preferred language is sign language. A decrease of 46 people (32%) since the 2011 Census
- 120 residents specifically use British Sign Language. A decrease of 35 people (29%) since the 2011 Census.
Sight loss
National
The RNIB identified that:
- as of March 2023, there was a total of 268,500 people registered blind or partially sighted in England, a 3% decrease compared to 2019 to 2020
- 1 in 5 people will experience sight loss during their lifetime in the UK and every day, 250 people will begin to lose their sight
- There were 20,330 new sight loss registrations in 2022/23 in England, a slight (3%) decrease compared to 2019/20
- Being "registered” with your local social services as ‘sight impaired’ or ‘severely sight impaired’ is optional, therefore, registration is not a measure of prevalence, it only indicates how many people have completed the registration process
- The number of people impacted by sight loss is widely predicted to increase dramatically by 2050 (with increasing age, numbers of people with diabetes), so the recent decrease in registrations is an unexpected trend - 2.7 million people will be living with sight loss in the UK by 2030 and 4million by 2050
- By 2050, the costs of sight loss to the UK economy are expected to rise to at least £33.5 billion per year
- Increased ophthalmology waiting times provide an additional risk factor associated with sight loss. NHS England waiting list figures for ophthalmology show that 615,100 people were waiting in December 2023. This represents people being referred for a first appointment with a consultant ophthalmologist, rather than wider ophthalmology waiting times for follow-up and monitoring
- Public attitudes have been identified as a key barrier for blind and partially sighted people with more than a third of blind and partially sighted people saying that they sometimes or frequently experience negative attitudes from the general public because of their sight loss. Learn more about sight loss statistics across the UK
Brighton & Hove
In 2022, 7,610 people were estimated to be living with sight loss in Brighton & Hove. With that number projected to rise to 8,710 by 2032. Of the 7,610 people living with sight loss, 1,255 are registered blind or partially sighted. RNIB Sight Loss Data Tool about sight loss [accessed in December 2024]
According to the GP patient survey data, 1% of adults in Brighton & Hove report blindness or partial sight, compared to 1.4% for England. This has remained similar for Brighton & Hove since 2012 but increased from 1.1% for England. The lower rate for the city is likely due to its younger age structure.
In 2020 to 2021, 65 people were issued with certificates of vision impairment in Brighton & Hove.
In the city, 47.9 new Certifications of Visual Impairment (CVI) per 100,000 people were issued in 2016 tot 2017 compared to 42.7 in England. In 2023 to 2024 the rate of new CVIs issued in Brighton & Hove had reduced to 21.5 per 100,000 and is around half that of England (43.5) with little change in England over the last decade.
Table 1: Number of people registered blind or partially sighted per 100,000 population, Brighton & Hove and England, 2022 to 2023
| Age | Brighton & Hove | England |
|---|---|---|
| People aged 65 to 74 | 622 | 533 |
| People aged 75+ | 2,549 | 3,031 |
Source: Office for Health and Improvement Disparities
The number of people aged 75 years or over registered blind or partially sighted in Brighton & Hove (2,549 per 100,000 population in 2022 to 2023,) has decreased from 4,687 in 2016/17. The rate of people aged 65 to 74 registered blind or partially sighted in the city (622 per 100,000) is higher than for England (533). [Withdrawn] Productive Healthy Ageing Profile: 2023 update.
Main causes of sight loss considered preventable
This section considers sight loss where the main causes are considered preventable.
Age Related Macular Degeneration (AMD)
Figure 3: Number of people with age related macular degeneration per 100,000 population aged 65 years or over, Brighton & Hove and England, 2010 to 2011 to 2022 to 2023
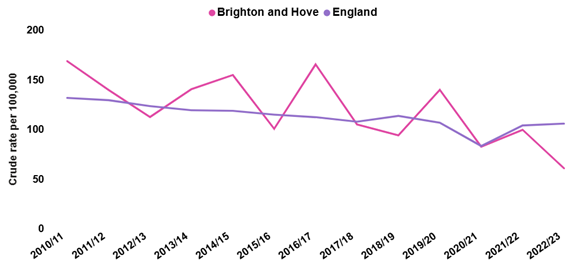
Source: Office for Health and Improvement Disparities, based on Moorfield Eye Hospitals and Office of National Statistics data
Since 2010 to 2011, the crude rate of new Certifications of Visual Impairment (CVI) due to age related macular degeneration (AMD), aged 65 plus per 100,000 population, for Brighton & Hove has fallen from 168.4 in 2010 to 2011 to was 60.7 in 2022 to 2023 (Figure 3).
Rates vary each year are the numbers of people with AMD are low, with 22 people recorded as having AMD in 2023 to 2024. (Office for Health Improvement and Disparities. Public health profiles) The rate has also fallen for England from 131.5 in 2010 to 2011 to 105.6 in 2022 to 2023.
Glaucoma
Numbers were suppressed for Brighton & Hove for 2022 to 2023 for new CVIs for glaucoma as below five. For 2021 to 2022, the rate of glaucoma in Brighton & Hove was 4.5 per 100,000 more than half that of England (12.6).
Diabetic eye disease (Diabetic retinopathy)
Numbers were suppressed for Brighton & Hove for the last five years for new CVIs for diabetic eye disease as below 5 each year.
Sight and hearing loss
- There are an estimated 250,000 people in the UK with both sight and hearing loss, with 88% of those with both sight and hearing loss aged 70 years or over.
- The RNIB estimate that 1,490 people are living with some degree of dual sensory loss in Brighton & Hove, with 610 of these individual living with severe dual sensory loss. (The Eyes Have It. Macular Society, Roche 2024)
Risk factors, impacts on health and wellbeing and prevention
Hearing loss
Causes of hearing loss
The RNID identifies that hearing loss may result from:
- age-related hearing loss, also known as presbycusis, is the most common cause of hearing loss is caused by changes that happen over time to the inner ear
- ear infections
- physical injury
- ototoxic medication: some medicines have side effects that can cause damage to the cochlea (hearing organ) or the balance system in the inner ear, which can lead to hearing loss, balance problems or tinnitus
- acoustic neuromas: a rare, slow-growing tumour on hearing and balance nerves
- Meniere’s disease: a rare inner ear condition that can affect balance and hearing. It cannot be cured, but treatment can help the symptoms
- genetic causes: in around 30% of children born with genetic hearing loss, the hearing loss is associated with other medical conditions or syndromes
- noise-induced hearing loss is caused by being around very loud sounds (find information about noise-induced hearing loss and regulations) like being in a noisy working environment* or listening to loud music
- loud bursts of sound, like gunshot or explosions
*Health and safety legislation places a duty of care on all employers to assess and identify measures to eliminate or reduce risks from exposure to noise to protect the hearing of employees, and to provide ongoing health surveillance.
Access to national and local data is not readily available for all of these potential causes of hearing loss.
Health and wellbeing impacts
Hearing loss affects communication, language development, and both educational and employment opportunities. Research indicates that people who use sign language have poorer economic status and lower educational attainment.
Without proper support, individuals may face growing exclusion from social interactions, leading to loneliness, isolation, and frustration. For elderly people, this can also result in poorer mental health and cognitive decline. NICE has recognised hearing loss as a major and growing public health challenge and recommended that the NHS do more to diagnose and manage adult hearing loss sooner.
Access to healthcare services and communication barriers with healthcare professionals have been linked to poorer health status and outcomes among Deaf BSL users. The first study of British Sign Language among deaf adults in the UK, conducted in 2015, revealed a higher prevalence of obesity, hypertension, and self-reported depression compared to the hearing population. Additionally, it highlighted an under-treatment of diabetes within this group. Most participants (53%) had no provision for a BSL interpreter during medical consultations, relying on lip-reading and posing serious constraints on their communication.
Sight loss
Causes of sight loss and risk factors
The leading causes of sight loss in the UK are:
The risk of sight loss is heavily influenced by health inequalities, deprivation and age, and other factors that increase the risk the risk of sight loss, including diabetes, hypertension and smoking. (Public health professionals)
Obesity
The rise in obesity rates, will lead to an increase in the number of people living with type 2 diabetes which will increase the risk of sight loss, as diabetes can cause various eye problems, including diabetic retinopathy, cataracts, and glaucoma.
Deprivation
The risk of sight loss and severe glaucoma are higher in people living in more deprived areas.
Find more information on the following websites
- Area deprivation, individual socioeconomic status and low vision in the EPIC-Norfolk Eye Study
- The effect of socio-economic deprivation on severity of glaucoma at presentation
- The relationship between multiple deprivation and severity of glaucoma at diagnosis
Ethnicity
There is a higher risk of sight loss in people from a White ethnic background as risk of sight loss is closely related to age, and ethnic minority groups in the UK have a younger average age. However, some ethnic groups are at a higher risk of developing some of the leading causes of sight loss at a younger age: Black African and Caribbean people are 4 to 8 times more at risk of developing certain forms of glaucoma and the risk of diabetic eye disease is about 3 times higher in South Asian people. People from minority ethnic backgrounds experience barriers to accessing eye health care, which can increase risk of avoidable sight loss.
Find more information on the following websites:
Gender
Two-thirds of the blind population in the world are female. Some factors (biological and socio-economical) are responsible for gender inequalities in eye health. Such as oestrogen provides a protective function against oxidation of the lens, thereby preventing cataracts and as the level of oestrogen reduces with age this may account for higher rates of cataracts in post-menopausal women.
(Doyal, L., Das-Bhaumik, R.G. 2018. Sex, Gender and Blindness: A New Framework for Equity. British Medical Journal of Open Ophthalmology [Online], 3:e000135. DOI: 10.1136/bmjophth-2017-000135 )
Smoking doubles the risk to sight in the following ways:
- causes harm to the tissues of the eye
- doubles the risk of developing AMD and developing the condition earlier.
- linked to the development of cataracts, and although treatable and do not lead to blindness, they remain a major cause of sight loss
- can make diabetes related sight problems worse as it reduces the flow of oxygenated blood in the peripheral vessels
- increases free radicals, which accelerate ageing, and alter the body's ability to absorb or extract necessary vitamins and minerals from food
- passive smoking is almost as harmful as smoking.
Hypertension
Diagnosing and treating hypertension in a timely way is important for preventing hypertensive retinopathy, as over time, high blood pressure can damage the blood vessels in the eyes and affect eyesight. Early signs of hypertensive retinopathy include blurred vision and headaches. More severe symptoms, like sudden vision loss and bleeding into the eye, are also possible. (Living with an Eye Condition)
Hypertension has also been implicated in the pathogenesis of glaucoma and age-related macular degeneration.
In Brighton & Hove:
National and local data is available for the main health factors that increase the risk of sight loss, which include diabetes, smoking, hypertension, obesity and deprivation and is summarised here.
Diabetes prevalence
Diabetes prevalence (17+ years from QOF*): for Brighton & Hove was 5% in 2023 to 2024 for patients over 17 years with diabetes mellitus as recorded on GP practice registers, lower than England (8%) and has been consistently lower since data was first available in 2012 to 2013. It is important to support people with diabetes to attend their regular diabetic eye screening, or this may result in higher levels of diabetic retinopathy.
*QOF= the quality outcome framework is a voluntary reward and incentive programme for standardising and improving quality of patient care. Data is collated annually as part of an additional contractual payment mechanism.
Smoking prevalence
Smoking prevalence (15+ years from QOF) has decreased both nationally and locally and is now 17% for Brighton & Hove in 2024 to 2025. This is significantly higher than the rate in the South East (12%) and England (14%).
There are significant inequalities in the city: 25% of those in the most deprived 20% of areas, compared to 9% of those in the least deprived 20% of areas smoke – but this absolute inequality gap has narrowed from a gap of 23 percentage points in 2012 to 16 percentage points in 2024.
Hypertension QOF prevalence
Hypertension QOF prevalence (all ages from QOF) in Brighton & Hove has been significantly lower than England since 2012 to 2013. In 2023 to 2024 the prevalence of hypertension in Brighton & Hove was 10%, compared to 15% for England.
Obesity prevalence
The prevalence of diabetes and hypertension are likely to rise with increasing obesity rates. Prevalence for overweight (including obesity) in adults was 60% in April 2024 for Brighton & Hove, below England (65%).
Deprivation
Parts of the city, including Whitehawk, Moulsecoomb, Hollingdean, and parts of Woodingdean, are among the 20% most deprived areas in England.
Health and wellbeing impacts
Sight loss can be linked to poor health, increase the risk of depression, falls and hip fractures, loss of independence and living in poverty:
Emotional wellbeing
People with sight loss are at a higher risk of experiencing emotional distress including depression, isolation and anxiety.
Appropriate support is important for people experiencing sight loss. Whist there are ongoing improvements in clinical treatments, less attention has been paid to the whole patient pathway, from pre- to post-diagnosis, and the support mechanism.
RNIB research finds that many individuals feel ill equipped to live with their sight loss and the increased risk of poor wellbeing, low confidence and the impact this has on daily life:
- only 17% of people experiencing sight loss were offered emotional support in relation to their deteriorating vision
- people with sight loss were more than twice as likely to have experienced difficulties with unhappiness or depression than the UK average
- nearly half of blind and partially sighted people feel moderately or completely cut off from the people and things around them.
Falls
In England, an estimated 232,000 people aged over 65 with sight loss experience a fall each year, with 110,000 of these falls directly linked to sight loss and 8,880 severe falls attributed to sight loss in this age group resulting in admissions to A&E departments annually (Learn more about sight loss statistics across the UK)
Falls can result in hip fractures, loss of independence, increasing isolation and living in poverty.
Information and exclusion
Despite legislation that aims to protect the rights of blind people and people with sight loss, the accessibility of products, information and services is still not an area where people with sight loss have equality of experience. Whether this is being able to independently read instructions on grocery packaging, being able to enjoy TV shows with audio description or getting information from health services in accessible formats, blind people and people with sight loss experience a significant information and inclusion gap.
Prevention
Preventing sight loss can help individuals maintain their independence and reduce the need for social care support that would be needed if sight were permanently lost. Research by the Royal National Institute for Blind People (RNIB) indicates that 50% of blindness and serious sight loss cases could be prevented with timely detection and treatment. (Public health professionals)
Sight loss is not an inevitable part of aging; prevention can be taken at all levels:
Primary prevention
Primary prevention linked to maintaining overall good health with prevention programmes to reduce obesity, increase exercise and stop smoking which may prevent or delay the onset of eye disease.
Secondary prevention
Secondary prevention central to maintaining vision or slowing the progression of diseases which can result in sight loss such as Diabetic Eye Screening and is dependent on the organisation and delivery of health services
Tertiary prevention
Tertiary prevention requires services and voluntary organisations to support people to live independently, provide additional help for people to adapt to living with their eye condition.
The research also suggests that the uptake of sight tests is lower than expected, especially in more deprived areas. Low uptake of sight tests and delays in accessing treatments can result in late detection of preventable conditions and increased sight loss due to delayed intervention.
Local inequalities
Children and young people
In January 2024, there were more male (96) than female (68) pupils in Brighton & Hove schools who had either a hearing or visual loss (59% males). Year 6 has the highest number of pupils (18) with hearing or visual loss or both, with five pupils in reception year being the lowest (Figure 4).
There is lack of data regarding sensory loss in relation to other protected characteristics than age and sex.
Figure 4: Number of pupils with hearing loss or visual loss, or both, as primary need, by school year in Brighton & Hove schools, January 2024
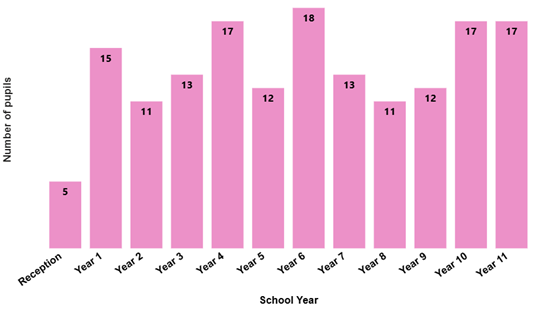
Source: School census data, January 2024.
Children and young people living with sensory loss experience a range of social and health inequalities which are evident in many areas of their lives, including access to services generally and specific sensory loss services; provision of appropriate accessible, including readable, information; opportunities for social engagement leading to isolation, and poorer health.
Find more information on the following websites:
- Sensory impairment – What it is, how it affects child development and how to help
- Identifying and supporting children and young people with sensory and/or physical needs: a rapid evidence review
Adults
The 2024 Health Counts survey of adults in Brighton & Hove provided rich data about the populations of Brighton & Hove, with analysis by sensory loss. The survey highlights that people with sensory loss (hearing loss or sight loss) face unique challenges that affect their well-being in several key areas compared to the total adult population in Brighton & Hove (B&H).[i
Data tables are available in Appendix1.
Healthy lifestyles
Physical activity
People with sensory loss are significantly less likely to engage in the recommended 30 minutes of sport and fitness activity in the last week (69% for hearing loss, 71% for sight loss, compared to 53% B&H)
Sedentary behaviour
People with sight loss are more likely to sit for 10+ hours on weekdays (30% for hearing loss, 37% for sight loss, compared to 28% B&H)
Time in nature
Adults with sensory loss spend less time in nature at least once a month compared to Brighton & Hove adults overall (81% for hearing loss, 80% for sight loss, compared to 89% B&H average)
Diet and healthy weight
While fruit and vegetable consumption are similar for adults with sensory loss when compared to the overall Brighton & Hove figures, adults with sensory loss are significantly less likely to have a healthy weight (25% for hearing loss, 25% for sight loss, compared to 37% Brighton & Hove)
Oral health
Adults with sensory loss are less likely to brush their teeth twice daily compared to Brighton & Hove overall (69% for hearing loss, 68% for sight loss, compared to 75% B&H), but the percentage of people with sensory loss who never attend a dentist is similar to overall city figure
Smoking, alcohol and drugs
People with hearing loss are less likely to smoke (12% compared to 17% Brighton & Hove), drink at increasing or higher risk levels (34% vs. 44% Brighton & Hove), or use drugs in the last year (12% compared to 20% Brighton & Hove). The figures are similar to the Brighton and Hove average for people with sight loss
Sexual health
Those with hearing loss who had sex with a new partner in the last year were significantly more likely to have never used a condom (37% compared to 16% Brighton & Hove)
Gambling, community safety, community cohesion, housing and cost of living
Gambling
People with hearing loss are more likely to gamble (26% compared to 22% Brighton & Hove overall) and, for those who gamble, to experience gambling related harms (27% compared to 19% Brighton & Hove overall)
Community safety
Feeling unsafe when out at night is a greater concern for people with sensory loss (43% hearing loss, 46% sight loss compared to 34% Brighton & Hove overall)
People with sensory loss are significantly more worried about being the target of hate crime because of their disability or assumed disability (12% hearing loss, 14% sight loss compared to 5% Brighton & Hove overall)
Community cohesion and connectedness
People with hearing loss report a stronger sense of belonging to their local area (62% hearing loss compared to 53% B&H) but was similar for those with sight loss (58%) to Brighton & Hove.
People with sensory loss are more likely to see or speak to their neighbours at least once or twice a week (68% hearing loss, 63% sight loss compared to 56% Brighton & Hove).
People with sight loss are less likely to have someone they can ask for help if they were ill in bed (60% compared to 70% Brighton & Hove), but was similar for those with hearing loss (69%) to the overall city figure.
Housing concerns and cost of living
Concerns about housing and taking action due to the cost of living are similar to the city overall figures.
Mental wellbeing
Happiness and anxiety
People with sight loss experience significantly lower happiness and higher anxiety levels (32% low happiness, 44% anxiety) compared to the Brighton & Hove overall (24% low happiness, 38% anxiety). Figures for those with hearing loss (26% low happiness, 39% anxiety) were similar to Brighton & Hove.
Suicide attempts and self-harm
People with sensory loss are more likely to have attempted suicide than the Brighton & Hove overall figure (17% hearing loss, 18% sight loss compared to 12% Brighton & Hove), rates of self-harm in the last 12 months was significantly lower in people with hearing loss (5% compared to 9% Brighton & Hove), but was similar for those with sight loss (10%) to the overall city figure.
Health Counts highlights the inequalities and discrimination experienced by people with hearing and sight loss in Brighton & Hove. Addressing these issues requires tailored interventions to support and improve physical activity levels, reduce gambling harms, enhance community safety, and provide appropriate mental health support. Efforts need to focus on creating more inclusive environments and tackling negative attitudes towards people with additional sensory support needs.
Local services and support for people with sensory loss
Brighton & Hove City Council commissions or provides:
- a specialist community support service with BSL trained support workers for d/Deaf people who have eligible needs under the Care Act 2014
- a specialist organisation for people with sight loss to provide social groups, support and wellbeing
- deaf advocacy so people can work with a BSL-trained advocate to say what they want or need in relation to their health or social care
- a specialist community equipment service that can support with aids and equipment in relation to sight or hearing loss.
- a team of Vision Rehabilitation Specialists providing support to people with sight loss, including registration and rehabilitation, information and advice.
Within the city there are also:
- the Sussex Eye Hospital provides eye A&E services and ophthalmology
- a local Eye Clinic Liaison Officer who supports & signposts people with sight loss
- over 20 specialist audiology businesses
- over 30 opticians offering a range of eye health and care services
- an increasing number provide both optometry and audiology services.
- several active local community and voluntary sector organisations that specifically support people with sensory loss in the city which can be found via the Community Works webpages.
Local treatment data
Hearing loss
At the time of writing, no data was available for appointments or treatments related to hearing loss, including specialised support, or for the provision of hearing aids either by health services or privately arranged.
Sight loss
A range of data is available for eye and vision related appointments and hospital treatments. Access to timely treatment can prevent further development of conditions that may impact on sight loss.
Vision outpatient attendances
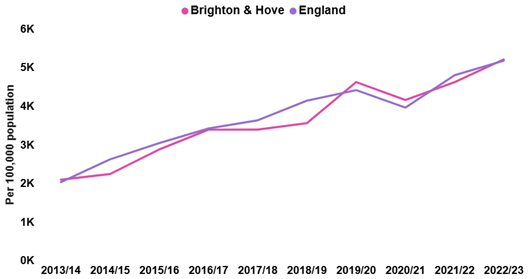
Brighton & Hove had a lower rate of vision outpatient attendances than England between 2013 to 204 and 2022 to 2023 (Figure 5).
In 2022 to 2023 the Brighton & Hove rate was 5,278 per 100,000, lower than England (5,801). COVID-19 impacted outpatient appointments, but rates have returned to near pre-Covid-19 levels.
Figure 5: Vision outpatient attendances (person based), directly age standardised rates per 100,000 for for all ages, Brighton & Hove and England, 2013 to 2014 to 2022 to 2023
Source: Office for Health Improvement and Disparities.
Due to the impact of coronavirus (COVID-19) on hospital activity, data relating to the financial year 2020 to 2021 should be interpreted with caution.
Vision procedures
Intravitreal injection therapy can be used to treat several conditions, including age-related macular degeneration*. The procedure rates have generally increased from approximately 2,000 per 100,000 for both Brighton & Hove and England in 2013 to 2014, to 5,205 for Brighton & Hove and 5,174 for England in 2022 to 2023 (Figure 6).
Cataract surgery
Cataracts are more common in older people than younger and impede sight. Cataract surgery involves replacing the lens and has a high success rate in improving eyesight. Whilst the causes are not considered preventable it requires timely diagnosis, monitoring and prompt treatment to prevent further sight loss. The rates of admissions to hospital for cataract surgery in people aged 65 years or over have increased for both Brighton & Hove and England between 2013 to 2014 and 2022 to 2023, for Brighton & Hove from 2,802 per 100,000 to 4,243, and for England from 3,277 per 100,000 to 4,679 (Figure 7).
*Plus Diabetic macular oedema, Retinal vein occlusion, and Inflammation or short-sightedness-related abnormal blood vessel growth. Anti-VEGF intravitreal injection treatment.
Figure 6: Intravitreal injection therapy procedures in people aged 60 years and over, directly age standardised rates per 100,000, Brighton & Hove and England, 2013 to 2014 to 2022 to 2023
Source: Office for Health Improvement and Disparities.
Figure 7: Admission to hospital for cataract surgery in people aged 65 years and over, directly age standardised rates per 100,000, Brighton & Hove and England, 2013 to 2014 to 2022 to 2023
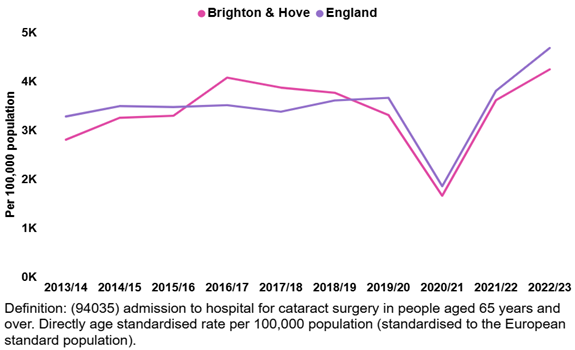
Source: Office for Health Improvement and Disparities.
Due to the impact of coronavirus (COVID-19) on hospital activity, data relating to the financial year 2020/21 should be interpreted with caution.
- Surgery to correct retinal detachment (rhegmatogenous surgery)
Brighton & Hove had a similar rate of surgery to correct retinal detachment (rhegmatogenous surgery) at 31.5 per 100,000 people aged 18 and over to England (25.9). Rates in both Brighton & Hove and England increased (excluding during Covid), from 22.5 and 18.3 per 100,000 respectively in 2013/14.
Social care and education data
Adult Social Care
Brighton & Hove City Council collects data for those using their services, for those using services commissioned from external organisations, and as Direct Payments for Personal Assistants.
Data for adult services in the financial year 2024 to 2025 show that:
- of all people receiving adult social care services, 302 had sight loss, 271 were D/deaf or hard of hearing, and 157 were listed as having another sensory need
- 21 people had sensory support as their primary support reason and of these six were aged 65 years or over
- of these 21 people;
- 7 received direct payments to fund services of their choice
- 13 people were funded for the specialist deaf community support service
- Fewer than five people had homecare support, were in residential or nursing care, or in supported living or extra care.
Access to suitable education
While majority of the children living with visual needs are educated in mainstream education in England, many are being deprived of specialist support due to disparities in service provision.
Statistics from Sense in 2022 shows that “Multi-sensory Impairment (MSI) specialist teaching provision varies widely across the country. There is a high percentage of areas without MSI teachers in the North-West (81%), compared with a low percentage in the South-East of England (27%)”. Children with multi-sensory impairment miss out on support.
In Brighton & Hove, the Sensory Needs Team (SNT) supports children with hearing or sight loss, their families, and teaching staff, in both mainstream and special schools. The team consists of teachers with specialist qualifications in hearing and/or visual impairment, an Educational Audiologist, a Family Support Worker, and a Mobility Officer. For deaf children not yet ready for mainstream schools, there is a specialist provision at Bevendean School.
Most children have a support package or an Educational Health and Care Plan (EHCP). Additionally, some children and young people with other health conditions may attend special schools or college. According to the schools’ census:
In January 2024 there were 85 children with hearing loss with SEN support and 20 with an EHCP with a primary need of sight loss. The number of children with an EHCP for hearing loss has remained similar (21 in 2020 to 24 children in 2024), as has the number with SEN support (83 and 85 respectively)
In January 2024 there were 42 children with sight loss with SEN support and 17 with an EHCP with a primary need of sight loss. The number of children with an EHCP (21 in 2020 to 24 children in 2024), for sight loss and SEN support (83 and 85 respectively) has remained similar.
Predicted future need
Both hearing and sight loss increase with age. Based on the Office for National Statistics population projections, between 2022 and 2032, the largest increase in population is projected in those aged 80 years or over (31% increase to 11,886 from 9,051 in 2022) and aged 60 to 69 years (29% increase to 32,557 from 25,287 in 2022).
Find this information on the following websites:
- Population and migration - Office for National Statistics
- JSNA Population in Brighton & Hove Executive Summary
By 2035, there will be a projected:
- 53,000 people in the city with a level of hearing loss that impacts upon their lives – an increase from 46,600 in 2025 with almost all of this increase in those aged 65 years or over (from 28,000 to 34,900)
- 6,100 people in the city with a level of sight loss that impacts upon their lives – an increase from 5,100 in 2025 with all of this increase in those aged 65+ years (an estimated 132 people aged under 65 years in both 2025 and 2035)
This estimate for those with sight loss is fewer than the RNIB data tool which predicts 8,700 people by 2032.
Full data tables available are in the Appendix 1.
What we don't know
There is a lack of local data relating to deafness and hearing loss, with numbers of people born deaf or with hearing loss difficult to describe at a local level. National antenatal and infant screening programmes and routine baby developmental checks collect data of hearing and sight in new-born and young children as they develop, which informs school entry but does not continue throughout the life course.
There are an increasing number of specialist audiology high street companies offering hearing tests and providing hearing aids as well as tests through the GP referral routes. Many large pharmacies and opticians have hearing specialists (audiologists) who offer hearing tests for adults aged 18 and over. The test is often free, although any treatment or hearing aids incur costs.
No NHS data was available on numbers of people tested and identified with hearing loss, the degree of loss, any treatments, and the number of hearing aids provided. This is also the case with privately paid for tests, aids etc, and some of this data may be considered commercially sensitive. The RNID provide a free hearing test online and collate data to inform their research.
There are a number of high street opticians offering free and paid for eye tests. The NHS funds opticians to provide free tests or optical vouchers to a range of people such as those aged 60 and over, people on certain benefits, those with family histories of eye conditions or people with diabetes.
NHS data on the number of people receiving these eye tests, or eye conditions diagnosed, or level of sight loss identified is not available. Data on the number of people paying for sight tests is commercially sensitive for the optician companies so is also not available.
Data on either d/Deaf people or people with sight loss with social care needs may not be reliable, particularly if people are experiencing significant barriers to accessing a social care assessment initially.